From first check-in to first plan: a practical HR response to burnout

Sam has been increasingly absent over the past few months. Deadlines slip. They’ve got less to say in meetings. They look tired in ways that no coffee can fix. Then they call in sick for three weeks. The team lead raises the possibility of burnout. HR now needs to schedule the first check-in call. This is the moment where good intentions either become real actions or just noise. It’s also where existing trust shows itself: employees don’t have to explain their absence, but when trust is there, they're more likely to share—and that’s what makes meaningful support possible.
PSST!
This Sam of ours is not just a fictional person, but three very real people we’ve talked to about their burnout experience for this report. Their stories are real. To avoid calling them out by name, we will refer to all three individuals experiencing burnout (and their insights) collectively as “Sam.”
Burnout is widespread enough that most leaders have seen the pattern before. Studies tell us that 63% of people today show at least one sign linked to burnout; things like exhaustion, mental distance from work, or a decline in performance. In practice, though, burnout is rarely recognized early. In many organizations, HR only becomes involved once something visible and disruptive happens (a breakdown, prolonged exhaustion, or a doctor signing someone off). At that point, the signals were often there for a long time, but they were normalized, explained away, or absorbed into “how things are right now.”
But still, when the first “burnout call” lands on the calendar, a lot of organizations still seem to improvise. They default to polite phrases, unclear roles, and processes that feel more like administration than actual support.
We want to change that, so we sat down with a group of HR leaders and a medical doctor to find the best way forward. Their insights have shaped this practical playbook, allowing other HR leaders and teams handling a suspected burnout case to use them—starting with the first call, and followed by the first 48 hours after that call. It’s designed for the moment when the situation has escalated and your next move really matters. Because, let’s be honest; there’s no shortage of burnout prevention content out there—but there is a lack of guidance for the moment when prevention has already failed.
Burnout starts with your workplace structure, it then becomes a health situation, and very quickly it’s turned into a business risk
Burnout is often talked about as a personal resilience issue. That framing tends to fail people. The WHO defines burnout as “an occupational phenomenon tied to chronic workplace stress that has not been successfully managed, marked by exhaustion, mental distance or cynicism, and reduced professional efficacy.”
That language matters a lot, because it changes how HR shows up. The best responses treat burnout as three different things, all at once.
It’s a human situation. Someone’s capacity has collapsed. They are not choosing this.
It’s a workplace design signal. Something about expectations, resources, and reality has drifted out of alignment.
Now, humanism and ethics aside here—this is a real business risk, with real costs attached.
“One of the most underappreciated features of burnout is that people usually still want to work. The problem is rarely motivation—it’s capacity. That gap is where burnout is often missed.”
Several HR leaders described this way of working not as a finished solution, but as an ongoing practice.
“We don’t see ourselves as having the perfect answer, but as people searching for a better version than last time. It’s a constant process of trying things out — it depends a lot on how close HR is to leadership, and how close leadership is to employees.” — Stephanie Filli, Deputy Head of Human Resources, Transa Backpacking AG
Workplace stress has been linked to $125–190 billion in additional healthcare spending in the U.S. alone, estimated at 5–8% of national health spending. In Switzerland, that number is CHF 7.6 billion—72%of which comes from employees who were present at work but not performing at full capacity.
“Some people think that burnout is just a mental state. But this type of prolonged stress triggers real biological changes in the body, too—from how the stress system is regulated to how the brain processes decision-making and emotion. At that point, this isn’t something a person can fix with more discipline or willpower. The body is under strain too, not just the mind. And that’s really important to remember.”
In other words: this is not a footnote topic. It’s also not solved by a single “check-in.”
The (actual) point of the first call
“In the first few minutes of a burnout-related call, it’s important to accept that you’re dealing with a multilayered situation you can’t fully understand yet. What’s really going on often only becomes clear over time.”
The first call has one purpose: create safety and clarity without adding pressure. It’s then up to you to establish a workable path for the next two days, and to put the right people and resources in motion.
“At the very start, there’s often a trust gap. Many employees see HR as ‘the company’—and the company is what made them sick. Before any process can land, the real work is rebuilding trust through transparency, confidentiality, and a calm explanation of the options they actually have.”
Many HR teams are tempted to use the first call to “get the facts.” They ask for timelines. They ask about return dates. They ask for details an employee probably doesn’t have. Sam described how pressure can creep in through seemingly normal questions after sick leave begins: unannounced check-ins, “How are you, what’s the prognosis, when are you coming back?” Questions they could not answer and did not want to face yet. The effect was more pressure and the feeling of still having to function—or otherwise lose their job.
“We can really only help when there’s a foundation of trust and transparency between everyone involved.” — Stephanie Filli, Deputy Head of Human Resources, Transa Backpacking AG
Treat the first call as a simple task: remove ambiguity, remove hidden expectations, and give the employee a sense that they are not alone in navigating what comes next.
The first 48 hours playbook
This section is intentionally specific. You can start following it tomorrow if you need to.
Get aligned internally before you contact the employee
Before you call Sam, run a short internal alignment.
Keep it small. Keep it calm. The goal is a shared plan, not a committee.
At the very least, decide 4 things:
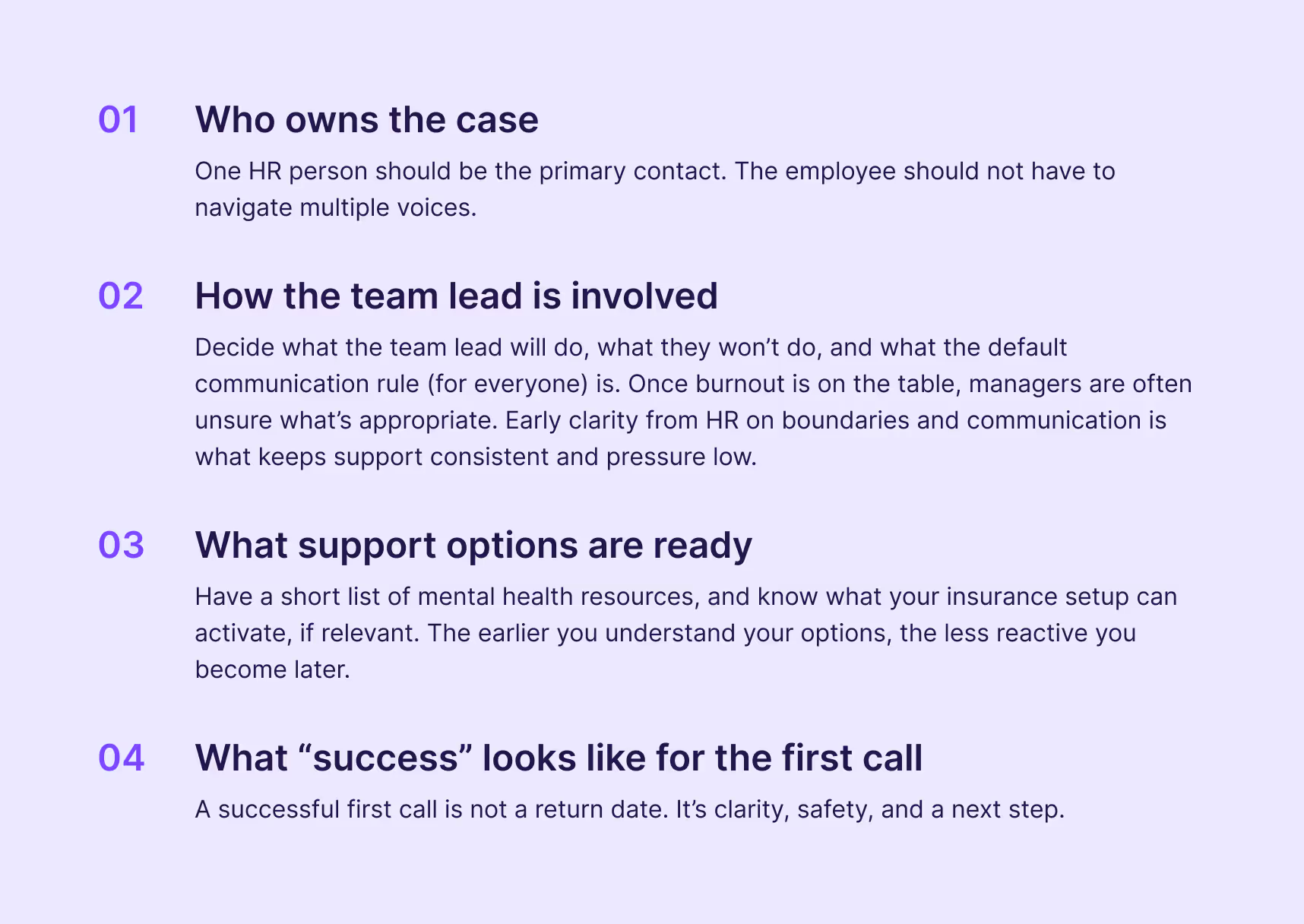
If you have an absence, claims, or occupational health person available; loop them in early enough that they can advise without taking over. When HR waits too long, it can turn into rushed handoffs later, when the employee is already depleted.
Prepare your call like you would for any high-stakes moment
Remember: You are not calling to “check in.” You are calling to set a tone and a structure. Before the call, take time to prepare a few core elements. This helps you stay grounded and helps the employee feel safe from the very first minute.
- Your opening sentence.
- The two things you will promise (and can actually deliver).
- The three questions you will ask.
- One clear, calming sentence you will repeat throughout the conversation to reinforce safety and clarity.
A lot of HR language sounds kind, but ends up shifting responsibility back onto the employee. Sam told us they often heard, before burnout, “We trust you to speak up if it gets too much.” On the surface, that sounds supportive. In reality, it places the burden of risk detection on the person already under strain.
Employers do carry responsibility for employee health to a certain extent. That responsibility isn’t met by waiting for someone to raise their hand. It shows up earlier than the breaking point—by noticing unsustainable workloads and acting on them. “Take care of yourself” can sound polite, but what actually helps is naming that three parallel projects are too much and deciding together what comes off the plate.
Run the first call with support-first language and clear boundaries

This is the moment where many organizations accidentally create pressure through politeness. Sam described feeling like the company sent gestures and questions, but not real seriousness. A “get well” message, then a growing sense that there was less interest in a return, less planability, and poor communication.
“In burnout cases, people often sound more functional than they really are. They tend to underestimate how depleted they are and overestimate how quickly they’ll recover. That’s why early support has to be based on observed capacity, not optimism.” — Dr. med. Mike Egloff, AcciMed GmbH
So you state the seriousness in practical ways: one point of contact, a predictable check-in rhythm, and clear protection from informal expectations.
Ask a small number of questions that reduce uncertainty.
- 01
“What kind of contact feels okay right now: email, phone, or nothing for a while?”
- 02
“Do you have someone supporting you medically and/or therapeutically?”
- 03
“Is there anything about work contact that would make things worse right now?”
“If the employee wants to share what led up to this, focus on listening rather than documenting. Stay present, notice how they react to what’s being said, and let the conversation breathe. Patterns and themes can be reflected on later, once things feel more settled.” — Semira Mayer, Psychologist and Product Manager at grape.
Close the chat with “next steps” that you own.
Summarize in plain language. Repeat your promises. Send a written recap. Keep it short.
Decide the colleague and team communication rule immediately
People often mean well. They also fill silence with assumptions. To avoid that, try to define the following things within the first 48 hours.
- Who communicates to the team
- What is said
- What is not said
- How (if at all) colleagues can reach out without creating pressure
“Just make sure to not speculate about an employee’s health. A burnout-related absence is a medical issue—not an HR discussion topic.” — Marcel Bahro, MD
A workable default is: colleagues can send one supportive message with no expectation of reply. No work updates. No “let me know if you need anything” phrasing that creates responsibility. Keep it simple and warm. You can even give your employees examples of what good/bad communication looks like at this sensitive moment.
Employment relationships run on trust and appreciation. So when someone disappears from the system without clear, respectful communication, trust disappears on both sides.
Document the case like it matters, because it does
Documentation tends to be treated as admin. In a burnout case, it’s part of your duty of care. It also protects the employee from memory drift later. Sam told us that, when returning to work, leadership claimed, “we didn’t know—why didn’t you say something?” Sam felt unheard over time, even while carrying visible load and raising structural issues.
Make sure to always document the takeaways of your chat(s).
- When concerns surfaced and what signals were visible
- What support was offered and when
- Who is responsible for what’s next
- What the employee requested around contact and privacy
Keep your notes factual and respectful. Avoid interpretations about motivation.
“What helps most is documenting functional observations—energy, clarity, consistency, and changes over time. That often gives a more accurate picture than any single conversation.”
Activate practical support early, not after the crisis becomes long-term
HR teams often default to “resources exist.” For someone already under strain, that can mean being left to navigate options alone. When support stays abstract, responsibility quietly shifts back to the employee when—in reality—it should be shared.
- 01Clinical care and recovery support.
- 02Work-directed adjustments.
- 03Insurance and case navigation.
If the employee has a therapist, that’s great. If they don’t, having options ready can remove a big barrier. Combining evidence-based clinical care with work-directed interventions like graded return-to-work programs and supported employment reduces mental health symptoms and sickness absence.
“One thing I’ve seen work before is mental health ambassadors—trained peers rather than managers—who can lower barriers to asking for help by reducing power dynamics and making support feel safer.” — Semira Mayer, Psychologist and Product Manager at grape
This includes workload reduction, removing high-pressure responsibilities, and shifting expectations. It also includes preparing accommodations, even if the immediate focus is sick leave. Employers in many places around the world have a legal duty to provide reasonable accommodations for employees with mental health conditions, including flexible hours, remote work options, leave for treatment, job restructuring, and adjustments to supervision methods.
In Switzerland, employers are expected to protect psychological health at work. Adjusting workload, expectations, and working conditions is often part of meeting that responsibility—even when the immediate focus is on recovery rather than return.
If your employee insurance and claims setup can support return-to-work planning or provide case management, knowing the pathway early reduces confusion later. The goal here is simple: fewer handoffs, fewer “you need to call this person,” and fewer moments where the employee has to coordinate their own recovery logistics.
“Uncertainty around pay and process creates huge stress. Explaining medical certificates, daily allowance cadence, payment changes, and who talks to the insurer early on is often one of the most effective forms of support HR can offer.”
3 Common mistakes in the first 48 hours (and what to do instead)
This is where many organizations tend to lose the plot. The good news is: you can avoid it.
Waiting too long because you don’t want to intrude
Silence feels respectful from the outside. From the inside, it can feel like abandonment. Sam described how the feeling of interest in their return got smaller over time, paired with a lack of planability and poor communication.
A good approach is early, explicit permission-based contact: one clear call, then an agreed rhythm. An even better approach is building trust and healthy relationships long before something happens in the first place.
Using “support” language that adds responsibility
The “good intentions” phrases are common because they sound kind. But they also tend to push responsibility back onto the employee.
“We trust you to speak up” sounds empowering for someone that’s currently strong and healthy. But for someone on the edge, it can also sound like: you failed to manage your own collapse. The alternative language moves responsibility into the system: “Let’s look at your workload together before it gets too much.”
If your language does not change expectations or load, it’s comfort without help.
Blurring roles between HR and the team lead
The team lead often cares deeply. That’s typically why they’re the team lead. But they may also be part of the conditions that created the burnout in the first place, even if it’s completely unintentionally.
So decide boundaries. HR owns the case management and duty of care process. The team lead supports relationally and operationally within HR’s structure. The employee should never feel like they have to “perform health” for their manager.
Why this matters beyond the individual case
A burnout case sits at the intersection of health, culture, and operations. It becomes visible when performance dips and absences rise. Oh, and it leaves a financial trail, too.
19% of U.S. workers rate their mental health as fair or poor, and those same workers report almost 12 days of unplanned absences per year compared to the 2.5 days for workers with better mental health. That gap reflects a practical reality: when mental health declines, the system pays in time, disruption, and churn.
The Swiss numbers underline the same point. In 2022, production losses linked to illness were estimated at CHF 70.5 billion, which is around 9% of Switzerland’s GDP. And in Zurich alone, more than CHF 2 billion in productivity was lost in 2024 due to health-related absences.

For a brand-led organization, there is another layer. Culture becomes credible in moments of strain. Employees remember the first call. They remember whether HR felt present, prepared, and human. Sam made this explicit: “work is a relationship that requires trust and appreciation.” When the system fails, people don’t just lose health. They lose trust in the relationship itself.
This is why this playbook is intentionally operational. Empathy becomes real when it shows up as structure.
What comes next: the three-month arc
The first call and first 48 hours create the foundation. The next weeks determine whether recovery is supported, delayed, or disrupted by workplace friction.
Let’s now cover the longer arc: how to work with insurance and claims at the right time, how to handle internal communication over weeks without drifting into silence, how to build a return-to-work program that employees can actually follow, and how to reduce relapse risk with better role alignment and workload design.
A good return-to-work program has clear roles and responsibilities, proactive communication, accommodation and support, education and training, and periodic review.
“Sustainable reintegration does not happen by chance – it is the result of clear responsibility, structured processes, and consistent support during periods of illness.”
From sick leave to return—setting up recovery that actually works
The first 48 hours set the tone. The following weeks decide whether recovery stabilizes or quietly unravels. This phase is less visible, more procedural, and often more decisive. It’s where systems either absorb stress or pass it back to the person who is already depleted.
We’ve made you a practical framework for the three-month arc starting after the initial call—focused on return-to-work design, coordination across functions, and reducing relapse risk without creating new pressure.
“Consistency is usually the first thing to slip. Early care fades, structure loosens, and responsibility gradually shifts back to the employee. Without active HR involvement, the same patterns that caused burnout tend to reappear.”
The middle phase: when intentions fade and structure matters more
After the first call, many organizations fall into a quiet waiting mode. HR waits for medical updates. Managers wait for HR. Colleagues wait for news. The employee waits, often without a clear sense of what is expected or when the next touchpoint will happen.
This gap is risky. It creates ambiguity, which is difficult to understand for someone recovering from burnout. It also increases the chance that return planning becomes rushed later. A stable middle phase has three characteristics: predictability, coordination, and visible responsibility.
Set up predictable contact without pressure
Agreeing on a contact rhythm sounds simple. In practice, it’s often skipped. What matters most here isn’t frequent contact, but predictable contact. Predictability means that the employee knows a few very important things—which reduces uncertainty and anxiety, especially when someone is already overwhelmed and doesn’t want untoward surprises.
- Who will contact them,
- how often,
- through which channel, and
- for what purpose.
A short written recap after each agreed check-in helps anchor this. Sending it to the employee allows for quick clarification and avoids misunderstandings. It removes the need for the employee to remember details or read between lines. Quarterly check-ins sound reasonable. A regular, safe space without consequence is what actually reduces anxiety and defensive behavior.
Coordination: fewer handoffs, clearer ownership
Burnout recovery often touches multiple functions.
- HR
- Line management
- Occupational health
- Insurance, claims and case management
- External clinicians
The risk here is fragmentation. Each actor does their part. The employee becomes the integrator. To avoid that, one function needs to hold the map. In most organizations, that role sits with HR. Not as a controller, but as a coordinator.
- They’re translating recovery-related guidance into work-relevant adjustments,
- aligning expectations between HR and managers, and
- timing insurance or claims involvement so it supports recovery rather than complicates it.
Combining clinical care with work-directed interventions, such as graded return-to-work programs and supported employment, reduces symptoms and sickness absence. The combination is the point. Clinical care alone does not redesign work.
“What makes a real difference is having one place that holds the full case view. When sick leave status, claims, payroll adjustments, and insurer communication are connected, HR can actually keep the overview—instead of chasing emails, PDFs, and updates from multiple sides. That frees up time to focus on the human part, not the paperwork.”
How to build return-to-work as a system, not an event
Return-to-work often gets treated as a date. That framing creates pressure and disappointment for everyone involved. A more realistic approach treats return-to-work as a staged process with built-in review points. This reduces all-or-nothing thinking and creates space for learning.
- A gradual increase in hours or scope
- Explicit workload boundaries
- Defined success markers for each phase
- A scheduled review to adjust course
Guidance on mental health return-to-work programs consistently highlights clear roles, proactive communication, accommodation, support for recovery, education, and periodic review as core elements. The design principle is simple: recovery fluctuates. Your plan definitely needs slack.
Why accommodation is not a concession
Accommodation is often discussed in legal terms. In practice, it’s a you-decision. Examples include flexible hours, temporary remote work, adjusted responsibilities, changes in supervision style, and protected time for treatment. In many jurisdictions, employers are required to provide reasonable accommodations for employees with mental health conditions, including these kinds of adjustments.
Beyond compliance, accommodations send a cultural signal. They say that health is compatible with contribution and that reintegration is protected, not scrutinized. This also reduces the likelihood of relapse, which carries real cost.
The role of the manager during reintegration
Managers often want to help. But they’re also under pressure to deliver. Without guidance, those pressures collide. In this phase, HR’s job is to equip managers with clarity.
- What has changed
- What remains off-limits
- How success will be evaluated during reintegration
This includes giving managers language. Sam’s experience of the contrast between praise and acknowledgment is really helpful: “You’re doing a great job, keep it up” can unintentionally push someone to overextend. Naming visible fatigue and offering shared load changes the dynamic.
Regular, short alignment points between HR and the manager help maintain consistency. They also prevent informal expectation creep.
How to learn without blame
A burnout case creates an opportunity to learn. It also creates defensiveness. Sam described a painful outcome: after their departure, the same structural issues remained at work. No deep dive happened. The system moved on unchanged.
“Burnout becomes easier to learn from when we stop looking at individual cases in isolation. Aggregated absence and health insights help shift the question from ‘what went wrong for this person?’ to ‘what in our system needs fixing?’”
Learning requires timing. Do not run a post-mortem while the person is still recovering. Do not wait so long that memory fades.
A constructive approach separates…
- individual recovery,
- role and workload design, and
- broader organizational patterns.
This keeps the focus on improvement rather than fault. It also respects the reality that burnout often comes from cumulative, normalized strain rather than just single failures.
Why brand and culture live here
For organizations that care about brand, this phase matters quietly and deeply. Employees talk less about policies and more about how situations were handled. The first call is remembered. The return is remembered even longer.
Workplace stress already carries massive external costs, estimated at $125–190 billion in additional healthcare spending in the U.S. alone. Internally, the cost shows up as disengagement, attrition, and loss of trust. Culture becomes credible when support is operational, predictable, and sustained. That credibility does not come from statements. It comes from your decisions.
Summary: Burnout response is organizational design
Burnouts can only be treated (and prevented) when organizations take responsibility for how work is structured, how pressure accumulates, and how recovery is supported. Not from goodwill alone. The first call creates safety. The first 48 hours create direction. And the following months test whether the system can hold someone while they heal.
Handled well, a burnout case can even strengthen trust and resilience. Handled poorly, it accelerates loss—of people, credibility, and institutional memory. It’s time we all treat burnout responses for what it is: a leadership challenge with real human lives stakes.
“In burnout cases, the most important factor was often having one trusted HR person throughout the process. Trust isn’t a given at the start. It’s built through transparency, clear communication, and consistency. I’ve seen that trust make the difference between disengagement and staying—even during sick leave.”